

Author’s note: I am grateful to the recently-launched caWsbar (Canadian Women’s Sex-based Rights) for bringing the McLean Clinic, and its aggressive marketing techniques, to my attention, as well as for files they contributed to this column. Dr. Alicia Hendley, Phd in psychology and founding member of caWsbar told me: “We’re very alarmed about the current trend of young women having double mastectomies to treat their dysphoria. We urge medical professionals to move beyond the external pressures they are being faced with and to put into action their most sacred principle—first do no harm.”
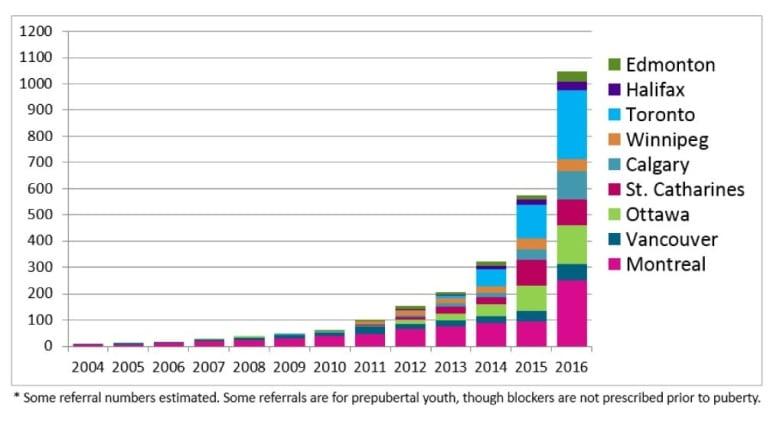
The rapid escalation of gender-fluid identification amongst young people in the West is nothing short of astounding. Adolescent females are now in a majority of those seeking transition. An Ottawa clinic, CHEO, used to see one or two patients a year. Last year it saw 189. It’s the same in other provinces:
Girls who are dissatisfied with their post-puberty bodies and wish to present as boys, naturally focus on their burgeoning breasts. They may use binders to flatten them, or they may seek surgical removal, referred to in the gender-fluidity world as “top surgery.”
Until fairly recently, a patient needed to undergo psychiatric testing before receiving OHIP approval for funding. Now a patient can be diagnosed by a GP or any other “expert” in gender health. Effectively, OHIP is now approving funding for any teenager who self-diagnoses as gender dysphoric, since Ontario law forbids any health professional from practicing “conversion therapy.” That is, any attempt by a doctor to inquire into contributing factors such as autism, anxiety, sexual preference, depression or other influencing factors could easily be construed as illegal.
The primary destination for top surgery in Ontario is the McLean Clinic, run by Dr. Hugh A. McLean, who has himself performed hundreds of top surgeries and who is not shy about promoting his clinic as a place where gender-fluidity dreams come true.
On the clinic’s Instagram page you can see dozens of photos of post-op FTM (female-to-male) clients posing bare-chested and happy. The clinic cheers on their patients—and prospective patients—with encouraging posts such as “Postop one day! What a way to start the holiday season. Nice job, Dr. McLean!” and “Ready for a topless summer.” Some of the females seem extremely young. Other adolescents comment, “I can’t wait to have this surgery too!” “I’m jealous!” In one photo, fellow surgeon Dr. Giancarlo McEvenue (more on him anon) wearing a mask and a Santa Claus hat holds up two buckets labelled “Breast tissue,” accompanied by a Dr McLean post: “For all you good boys, Dr McEvenue is not bringing gifts, he’s taking them away!”

We already know that adolescence is a notoriously labile period in the maturation cycle, and that teenagers under the age of 18 (at a minimum—our brains are not fully mature until 25) cannot be assumed to be making momentous decisions with truly “informed consent.” This Instagram page straddles a line between affirmation and recruitment.
Dr. McEvenue, Dr. McLean’s (until recently) colleague at the McLean clinic (he is listed as a surgeon here now), is as well a paid consultant for Johnson & Johnson, whose products and services are employed in these surgeries. Under their sponsorship, Dr. McEvenue participated in a gender reassignment surgery panel last September in Markham, Ontario. You can watch the panel and his performance here.
In the video, you see a marked transformation in Dr. McEvenue’s pitch. He’s jettisoned the Instagram-friendly Santa hat and the buckets of breast tissue. He is now the smooth, Madman-esque embodiment of Corporate Guy, representing a mammoth company that brands itself as so LGBT-friendly they are bursting with Pride and self-congratulation.
Dr. McEvenue tells us that there could be as many as two million people with gender dysphoria in Canada – about 1.5% of the population – considerably more than the DSM-5’s estimation of .002-.003%. Not only is the wish for top surgery not indicative of a disorder, he says, but it is even “not a distress,” and in fact it may not be necessarily exclusively related to gender dysphoria. Sometimes it is just “breast dysphoria,” he says, a term new to me, which turns out to mean that “you don’t like your breasts.” If that is your issue, Dr. McEvenue is there for you, and will remove them. Because he has a “passion” for what he does.
At the 14:30 minute mark, Dr. McEvenue inadvertently demonstrates the health community’s general dumbing-down of the transition process that he is abetting.
He says, “Believe it or not, when a patient wanted top surgery five or ten years ago, they had to go to a psychiatrist to get diagnosed.” (Here he grins, presumably at the craziness of the very idea that a woman wanting to lop her breasts off might benefit from sorting through her motives with a mental health expert). He continues, “If a woman comes to me for breast augmentation, I don’t make her go to a psychiatrist. I say, okay, are you an adult? Do you understand the surgery?” (laughter, applause. This audience really really wants to believe that top surgery on teenage girls is no big deal.)
So let’s unpack these statements. Dr. McEvenue is comparing breast removal to breast augmentation as though they were two sides of the same coin. But they’re not. The parallel to a breast augmentation is a breast reduction. Both surgeries are performed on women who identify as women, but for reasons of comfort (reduction) or perceived enhanced sexual allure (augmentation), seek surgical alterations. Of course such women do not require psychiatric evaluations. How is augmentation in any way logically comparable to top surgery for transitioning girls who want their breasts removed so they can present as male? It isn’t, unless you are attempting to trivialize both the operation and its psychological implications.
Furthermore, he asks his augmentation patients, “are you an adult?” But from the photos on the Instagram account, a great number of Dr. McEvenue’s patients are not adults at all. How does he know they truly understand what they are doing? Why wouldn’t he want them to see a psychiatrist beforehand? If they are sure of what they are doing, what harm can deeper exploration do? And if they are not sure, what’s the down side of them changing their mind? There is a long waiting list at the McLean Clinic, according to Dr. McEvenue. If one or two drop off it after consulting with a mental-health expert, where’s the tragedy there? Dr. McEvenue claims it is a matter of “respect” not to challenge his patients’ self-diagnosis. And at the 18-minute mark, he says, “Why would I send [a patient] for a second opinion?” Yet “second opinions” are standard in every other field of surgery, and no other surgeons consider them a sign of disrespect. (I guess it’s a good thing Dr. McEvenue isn’t an oncologist.)
Dr. McEvenue enthuses about the benefits of Instagram (“Instagram has been huge for us”) and boasts of the clinic’s 14,000 followers. He claims that he doesn’t moderate the discussion generated, although, “If I see a negative comment, I delete it.” The McLean Clinic is certainly dedicated to FTM transitioning as a “fun” experience.
Representing the patient experience on the panel is a likable transman, Yuri, who is warm, amiable and articulate, clearly at home in his new persona and eager to extol the benefits of his top surgery. Notably, he is now 30 years old, and had the surgery in his 20s. So he is hardly representative of the growing demographic that is seeking the surgery. If all the clinic’s patients were in their 20s, this panel wouldn’t have been needed. The subject is only controversial because the age of those undergoing it is moving downward. Parents are of course concerned, confused and occasionally desperate for objective advice.
They won’t find objectivity on this panel. Two of the speakers, the J & J host and Dr. McEvenue, are stakeholders in the business end of top surgeries. One of the panellists is a mature patient who had gone through years of reflection as an adult before doing it, and the last panellist, Melissa, is the parent of a child to whom she has given her full affirming support since her (then) daughter was four years old and refused to dress in princess clothes.
Melissa, unfortunately, plays the “suicide” card, saying, “I’d rather stand beside my son than over top of his grave.” Suicide is a “big possibility,” Melissa says, and a parent’s job “isn’t to understand, it’s to support” the dysphoric child. Dr. McEvenue reinforces her message with, “a lot of time this is a life-saving operation.” But since he is committed never to second-guessing the patient’s self-diagnosis, he cannot be sure that psychiatric help wouldn’t be equally life-saving.
Brown University researcher Lisa Littman, who coined the term “Rapid Onset Gender Dysphoria” (ROGD) found that many adolescent girls with problems other than gender dysphoria—autism, anxiety, depression—glommed on to gender dysphoria as the source of their troubles through sites like Reddit and Tumblr, where “social contagion” took hold of them. These sites school new adherents in the kind of tropes—such as threatening suicide—that are sure to get their parents on board and assure instant affirmation from therapists. Parents should know this.
So just how real is the risk of suicide if a young girl does not get her double mastectomy? In a very recent article published in Quillette, psychoanalyst Marcus Evans, who formerly served as Consultant Psychotherapist and Associate Clinical Director of Adult and Adolescent Service at the Tavistock and Portman NHS Trust, the Tavistock Clinic being England’s premier public gender clinic, has this to say on the subject of suicide risk: “Those who advocate an unquestioning ‘affirmation’-based approach to trans-identified children often will claim that any delay or hesitation in assisting a child’s desired gender transition may cause irreparable psychological harm, and possibly even lead to suicide. They also typically will cite research purporting to prove that a child who transitions can expect higher levels of psychological health and life satisfaction. None of these claims align substantially with any robust data or studies in this area. Nor do they align with the cases I have encountered over decades as a psychotherapist.”
What else is missing from this panel presentation? Questions that weren’t puffballs. For example, nobody asked whether Dr. McEvenue had ever had to reconstruct breasts after a client felt regret over the top surgery? (The McLean Clinic website says that “very few trans folk regret their decision to undergo top surgery as part of their transition to their experienced gender,” but they do not reference any studies.) Regretful detransitioners abound, and many of them want to be heard, but trans activists make life difficult for them when they speak out. Or another unasked question: Do you talk to these adolescent girls about their sexual preferences before planning their surgeries? Some girls presenting as trans are in fact merely lesbians who have difficulty processing that notion. In such cases, transitioning is neither required or advisable. But the subject did not arise on the panel.
As noted in a balanced, in-depth Atlantic magazine article on the subject by seasoned researcher Jesse Singal, the American Psychological Association’s guidelines observe that “adolescents can become intensely focused on their immediate desires.” It goes on: “This intense focus on immediate needs may create challenges in assuring that adolescents are cognitively and emotionally able to make life-altering decisions.” The McLean Clinic is marketing itself to this demographic, and far from appearing to see “challenge” in this demographic’s vulnerability, they show every sign of seeing only market opportunity.
It will be clear to any objective observer that the McLean Clinic’s “fun” approach to top surgery and its dependence on social media promotes a perspective that underplays the complexity of the issue and overplays the magical-solution angle. The McLean Clinic’s bruited compassion for their patients is commendable. But their Instagram culture makes a mockery of the “informed consent” they claim to respect.
From a business perspective, the Mclean Clinic’s long waiting list is a sign of success. Their marketing techniques are not illegal. But are they ethical? That is a subject the Canadian Society of Plastic Surgeons might wish to take under deliberation.
Join and support independent free thinkers!
We’re independent and can’t be cancelled. The establishment media is increasingly dedicated to divisive cancel culture, corporate wokeism, and political correctness, all while covering up corruption from the corridors of power. The need for fact-based journalism and thoughtful analysis has never been greater. When you support The Post Millennial, you support freedom of the press at a time when it's under direct attack. Join the ranks of independent, free thinkers by supporting us today for as little as $1.
Remind me next month
To find out what personal data we collect and how we use it, please visit our Privacy Policy






